Creating medication intelligence that actually works in the real world has always been a delicate balancing act. For patients and the clinical teams who support them, we viewed simplicity as the highest priority: the technology should feel intuitive and natural, fitting into routines rather than reshaping them. But given our goal of leapfrogging the proxy-event approaches that have dominated this category, a high degree of technical complexity across the system was always to be expected. Yet if that complexity complicated the patient or clinician experience, the product was likely to flop. This tension ultimately shaped everything that reached the people who use it, and navigating it occupied much of our team's thinking as we developed MyAide.
Some background helps frame the challenge. In an era of increasing reliance on telemedicine and remote patient monitoring, we saw a need for medication intelligence that could measure compliance with precision and put that information in front of clinicians and pharmacists in a form they could act on. What we built is a complete system rather than a single device: a smart dock and cap that measure medication use gravimetrically, a companion smartphone app for patients, and a set of dashboards for clinician and pharmacist workflows. Intelligence here is not just measurement. It is the whole loop, from what happens at the patient's counter to what shows up in a clinical workflow. For that loop to be useful, every part has to function together reliably and seamlessly.
What kept us honest throughout was a parallel commitment to simplicity of user experiences even while we welcomed technical complexity. Smart health products are nearly always grudge purchases. Patients only use them because they are dealing with a condition that already creates obstacles in their daily life, which leaves them with a very low tolerance for additional impositions. The same logic applies to the clinicians and clinical operations staff who interact with the system on the other end of the data. Our goal was to impose no further burden on either group. In practice, this meant that every time we added intelligence to the system, we measured the resulting experience against what performing that task would feel like without the technology at all. Sometimes complexity was clearly warranted, as when we built automatic data transmission so patients would not need to take any extra steps beyond using their medication. Other times, evaluating design ideas against real-life behavior made it immediately clear when we were asking too much of the user. Multiple rounds of feedback, from clinical experts at one end and everyday patients at the other, were essential to keeping that balance. Those additional iterations took time and effort, often delaying our updates by a few months. The pressure was not easy to take, for a startup, but we had no way to compromise.
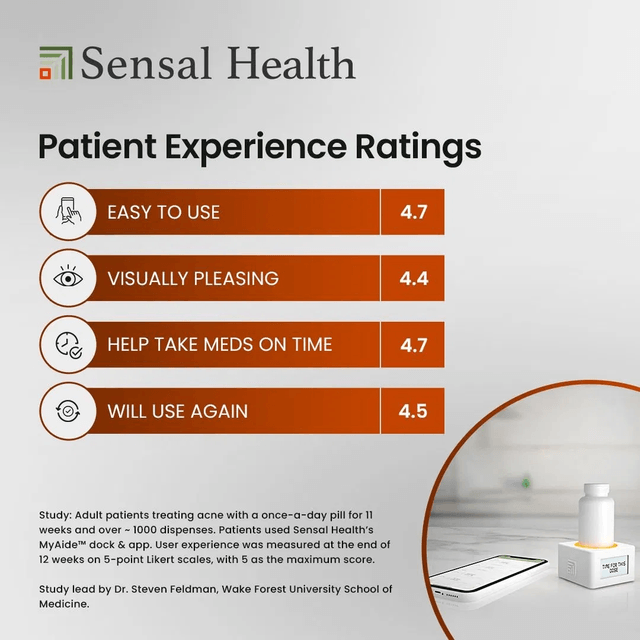
The patient experience ratings we received at the end of a recent study are, frankly, gratifying. On a five-point scale, patients rated the system 4.7 for ease of use and for helping them take their medication on time, 4.5 for likelihood to use again, and 4.4 for being visually pleasing. Those numbers tell us we threaded the needle, at least well enough that patients found the intelligence helpful rather than burdensome. Qualitative feedback, comments during zoom calls, and other feedback from clinicians and operators have been no less important in giving us a shared sense of rewards.
The line from idea to product almost never follows a simple path, and balancing a patient's need for simplicity against the demands of building genuine intelligence is a significant challenge. But success is attainable with a steady vision and shared principles to guide the process.