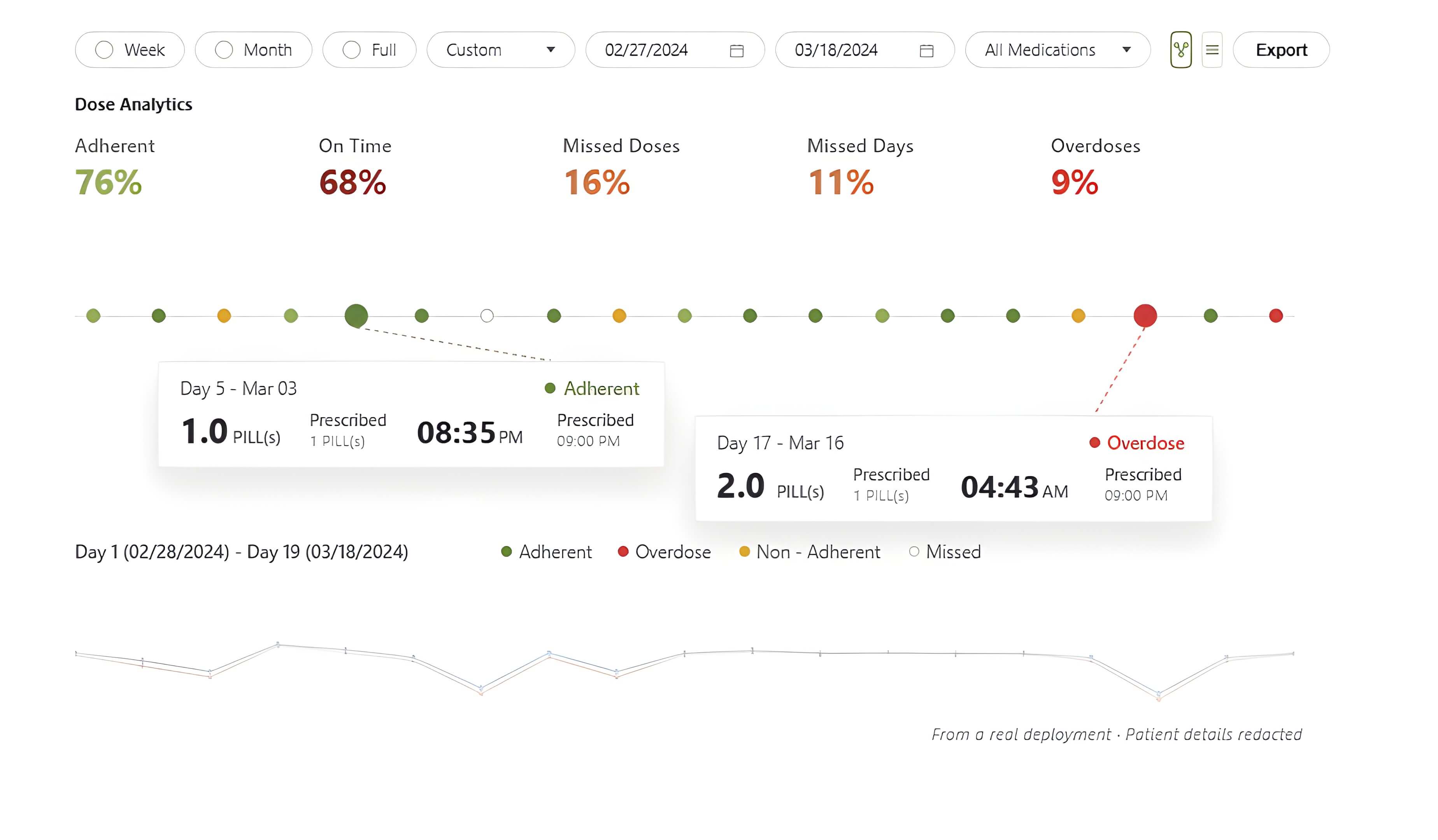
Verified
Overdose
Missed
Proxy tech · Pill cap
Dose taper failure.
2 tablets daily, days 1–5.
Taper to 1 tablet, days 6–7.
Patient does not taper.
| D1 | D2 | D3 | D4 | D5 | taper D6 |
D7 | |
|---|---|---|---|---|---|---|---|
| Prescribed | 2 | 2 | 2 | 2 | 2 | 1 | 1 |
| Actual | 2 | 2 | 2 | 2 | 2 | 2 | 2 |
| Proxy | |||||||
| MyAide | 2 | 2 | 2 | 2 | 2 | 2 | 2 |
Proxy monitor
Taper failure invisible. Full compliance reported.
MyAide
Overdose flagged days 6–7. Clinician alerted before day 8.